Frontal lobe
| The frontal Lobe | |
|---|---|
|
Principal fissures and lobes of the cerebrum viewed laterally. (Frontal lobe is shown in blue.) | |
 | |
| Details | |
| Part of | Cerebrum |
| Artery |
Anterior cerebral Middle cerebral |
| Identifiers | |
| Latin | Lobus frontalis |
| Acronym(s) | FL |
| MeSH | A08.186.211.730.885.213.270 |
| NeuroNames | hier-37 |
| NeuroLex ID | Frontal Lobe |
| TA | A14.1.09.110 |
| FMA | 61824 |

The frontal lobe, located at the front of the brain, is one of the four major lobes of the cerebral cortex in the mammalian brain. The frontal lobe is located at the front of each cerebral hemisphere and positioned in front of the parietal lobe and above and in front of the temporal lobe. It is separated from the parietal lobe by a space between tissues called the central sulcus, and from the temporal lobe by a deep fold called the lateral sulcus also called the Sylvian fissure. The precentral gyrus, forming the posterior border of the frontal lobe, contains the primary motor cortex, which controls voluntary movements of specific body parts.
The frontal lobe contains most of the dopamine-sensitive neurons in the cerebral cortex. The dopamine system is associated with reward, attention, short-term memory tasks, planning, and motivation. Dopamine tends to limit and select sensory information arriving from the thalamus to the forebrain. A report from the National Institute of Mental Health says a gene variant that reduces dopamine activity in the prefrontal cortex is related to poorer performance and inefficient functioning of that brain region during working memory tasks, and to a slightly increased risk for schizophrenia.[1]
Structure

On the lateral surface of the human brain, the central sulcus separates the frontal lobe from the parietal lobe. The lateral sulcus separates the frontal lobe from the temporal lobe.
The frontal lobe bottom can be divided into a lateral, polar, orbital (above the orbit; also called basal or ventral), and medial part. Each of these parts consists of particular gyri:
- Lateral part: lateral part of the superior frontal gyrus, middle frontal gyrus, inferior frontal gyrus.
- Polar part: Transverse frontopolar gyri, frontomarginal gyrus.
- Orbital part: Lateral orbital gyrus, anterior orbital gyrus, posterior orbital gyrus, medial orbital gyrus, gyrus rectus.
- Medial part: Medial part of the superior frontal gyrus, cingulate gyrus.
The gyri are separated by sulci. E.g., the precentral gyrus is in front of the central sulcus, and behind the precentral sulcus. The superior and middle frontal gyri are divided by the superior frontal sulcus. The middle and inferior frontal gyri are divided by the inferior frontal sulcus.
In humans, the frontal lobe reaches full maturity around the late 20s,[2] marking the cognitive maturity associated with adulthood. A small amount of atrophy, however, is normal in the aging person’s frontal lobe. Fjell, in 2009, studied atrophy of the brain in people aged 60–91 years. The 142 healthy participants were scanned using MRI. Their results were compared to those of 122 participants with Alzheimer's disease. A follow-up one year later showed there to have been a marked volumetric decline in those with Alzheimer's and a much smaller decline (averaging 0.5%) in the healthy group.[3] These findings corroborate those of Coffey, who in 1992 indicated that the frontal lobe decreases in volume approximately 0.5%–1% per year.[4]
Function
The frontal lobe plays a large role in voluntary movement. It houses the primary motor cortex which regulates activities like walking.
The function of the frontal lobe involves the ability to project future consequences resulting from current actions, the choice between good and bad actions (or better and best) (also known as conscience), the override and suppression of socially unacceptable responses, and the determination of similarities and differences between things or events.
The frontal lobe also plays an important part in integrating longer non-task based memories stored across the brain. These are often memories associated with emotions derived from input from the brain's limbic system. The frontal lobe modifies those emotions to generally fit socially acceptable norms.
Psychological tests that measure frontal lobe function include finger tapping (as the frontal lobe controls voluntary movement), the Wisconsin Card Sorting Test, and measures of language and numeracy skills.[5]
Clinical significance
Damage
Stuss, et al. discuss in a review of many studies how damage to the frontal lobe can occur in an assortment of ways and result in many different consequences. Transient ischemic attacks (TIAs) also known as mini-strokes, and strokes are common causes of frontal lobe damage in older adults (65 and over). These strokes and mini-strokes can occur due to the blockage of blood flow to the brain or as a result of the rupturing of an aneurysm in a cerebral artery. Other ways in which injury can occur include head injuries such as traumatic brain injuries incurred following accidents, diagnoses such as Alzheimer's disease or Parkinson's disease (which cause dementia symptoms), and frontal lobe epilepsy (which can occur at any age).[6]
Symptoms
Common effects of damage to the frontal lobe are varied. Patients who have experienced frontal lobe trauma may know the appropriate response to a situation but display inappropriate responses to those same situations in "real life". Similarly, emotions that are felt may not be expressed in the face or voice. For example, someone who is feeling happy would not smile, and his or her voice would be devoid of emotion. Along the same lines, though, the person may also exhibit excessive, unwarranted displays of emotion. Depression is common in stroke patients; it affects a great number of those who have experienced one. Also common along with depression is a loss of or decrease in motivation. Someone might not want to carry out normal daily activities and would not feel "up to it".[6] Those who are close to the person who has experienced the damage may notice that the person no longer behaves like him or herself.[7] This personality change is characteristic of damage to the frontal lobe and was exemplified in the case of Phineas Gage. The frontal lobe is the same part of the brain that is responsible for executive functions such as planning for the future, judgment, decision-making skills, attention span, and inhibition. These functions can decrease drastically in someone whose frontal lobe is damaged.[6]
Consequences that are seen less frequently are also varied. Confabulation may be the most frequently indicated "less common" effect. In the case of confabulation, someone gives false information while maintaining the belief that it is the truth; he or she cannot remember the accurate information. In a small number of patients, uncharacteristic cheerfulness can be noted. This effect is seen mostly in patients with lesions to the right frontal portion of the brain.[6][8]
Another infrequent effect is that of reduplicative paramnesia, in which patients believe that the location in which they currently reside is a replica of one located somewhere else. Similarly, those who experience Capgras syndrome after frontal lobe damage believe that an identical "replacement" has taken the identity of a close friend, relative, or other person and is posing as that person. This last effect is seen mostly in schizophrenic patients who also have a neurological disorder in the frontal lobe.[6][9]
History
Psychosurgery
In the early 20th century, a medical treatment for mental illness, first developed by Portuguese neurologist Egas Moniz, involved damaging the pathways connecting the frontal lobe to the limbic system. Frontal lobotomy (sometimes called frontal leucotomy) successfully reduced distress but at the cost of often blunting the subject's emotions, volition and personality. The indiscriminate use of this psychosurgical procedure, combined with its severe side effects and a mortality rate of 7.4 to 17 per cent,[10] gained it a bad reputation. The frontal lobotomy has largely died out as a psychiatric treatment. More precise psychosurgical procedures are still used, although rarely. They may include anterior capsulotomy (bilateral thermal lesions of the anterior limbs of the internal capsule) or the bilateral cingulotomy (involving lesions of the anterior cingulate gyri) and might be used to treat otherwise untreatable obsessional disorders or clinical depression.
Theories of function
Theories of frontal lobe function can be separated into four categories:
- Single-process theories, which propose that "damage to a single process or system is responsible for a number of different dysexecutive symptoms” [11]
- Multi-process theories, which propose "that the frontal lobe executive system consists of a number of components that typically work together in everyday actions (heterogeneity of function)" [12]
- Construct-led theories, which propose that "most if not all frontal functions can be explained by one construct (homogeneity of function) such as working memory or inhibition" [13]
- Single-symptom theories, which propose that a specific dysexecutive symptom (e.g., confabulation) is related to the processes and construct of the underlying structures.[14]
Other theories include:
- Stuss (1999) suggests a differentiation into two categories according to homogeneity and heterogeneity of function.
- Grafman's managerial knowledge units (MKU) / structured event complex (SEC) approach (cf. Wood & Grafman, 2003)
- Miller & Cohen's integrative theory of prefrontal functioning (e.g. Miller & Cohen, 2001)
- Rolls's stimulus-reward approach and Stuss's anterior attentional functions (Burgess & Simons, 2005; Burgess, 2003; Burke, 2007).
It may be highlighted that the theories described above differ in their focus on certain processes/systems or construct-lets. Stuss (1999) remarks that the question of homogeneity (single construct) or heterogeneity (multiple processes/systems) of function "may represent a problem of semantics and/or incomplete functional analysis rather than an unresolvable dichotomy" (p. 348). However, further research will show if a unified theory of frontal lobe function that fully accounts for the diversity of functions will be available.
In other animals
For many years, many scientists thought that the frontal lobe was disproportionately enlarged in humans compared to other primates. They thought that this was an important feature of human evolution and was the primary reason why human cognition differs from that of other primates. However, this view has been challenged by newer research. Using magnetic resonance imaging to determine the volume of the frontal cortex in humans, all extant ape species and several monkey species, Semendeferi et al. found that the human frontal cortex was not relatively larger than the cortex of other great apes but was relatively larger than the frontal cortex of lesser apes and the monkeys.[15]
Additional images
 Left frontal lobe (click to view animation)
Left frontal lobe (click to view animation) Lobes
Lobes Base of brain.
Base of brain.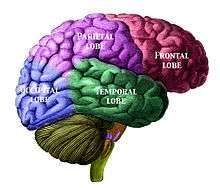 Human brain showing the four major lobes of the cerebrum. Beneath the cerebral cortex are the cerebellum, pons, olive, and medulla oblongata
Human brain showing the four major lobes of the cerebrum. Beneath the cerebral cortex are the cerebellum, pons, olive, and medulla oblongata Drawing to illustrate the relations of the brain to the skull.
Drawing to illustrate the relations of the brain to the skull. Frontal lobe
Frontal lobe Frontal lobe
Frontal lobe Cerebrum.Inferior view.Deep dissection
Cerebrum.Inferior view.Deep dissection Ventricles of brain and basal ganglia.Superior view. Horizontal section.Deep dissection
Ventricles of brain and basal ganglia.Superior view. Horizontal section.Deep dissection
See also
References
- ↑ "Gene Slows Frontal Lobes, Boosts Schizophrenia Risk". National Institute of Mental Health. May 29, 2001. Retrieved 2013-06-20.
- ↑ Giedd JN, Blumenthal J, Jeffries NO, et al. (October 1999). "Brain development during childhood and adolescence: a longitudinal MRI study". Nature Neuroscience. 2 (10): 861–3. doi:10.1038/13158. PMID 10491603.
- ↑ Fjell AM, Walhovd KB, Fennema-Notestine C, et al. (December 2009). "One-year brain atrophy evident in healthy aging". The Journal of Neuroscience. 29 (48): 15223–31. doi:10.1523/JNEUROSCI.3252-09.2009. PMC 2827793
 . PMID 19955375.
. PMID 19955375. - ↑ Coffey CE, Wilkinson WE, Parashos IA, et al. (March 1992). "Quantitative cerebral anatomy of the aging human brain: a cross-sectional study using magnetic resonance imaging". Neurology. 42 (3 Pt 1): 527–36. doi:10.1212/wnl.42.3.527. PMID 1549213.
- ↑ Kimberg DY, Farah MJ (December 1993). "A unified account of cognitive impairments following frontal lobe damage: the role of working memory in complex, organized behavior". Journal of Experimental Psychology. General. 122 (4): 411–28. doi:10.1037/0096-3445.122.4.411. PMID 8263463.
- 1 2 3 4 5 Stuss DT, Gow CA, Hetherington CR (June 1992). "'No longer Gage': frontal lobe dysfunction and emotional changes". Journal of Consulting and Clinical Psychology. 60 (3): 349–59. doi:10.1037/0022-006X.60.3.349. PMID 1619089.
- ↑ Rowe AD, Bullock PR, Polkey CE, Morris RG (March 2001). "'Theory of mind' impairments and their relationship to executive functioning following frontal lobe excisions". Brain. 124 (Pt 3): 600–16. doi:10.1093/brain/124.3.600. PMID 11222459.
- ↑ Robinson RG, Kubos KL, Starr LB, Rao K, Price TR (March 1984). "Mood disorders in stroke patients. Importance of location of lesion". Brain. 107 (1): 81–93. doi:10.1093/brain/107.1.81. PMID 6697163.
- ↑ Durani, Shiban K.; Ford, Rodney; Sajjad, S. H. (September 1991). "Capgras syndrome associated with a frontal lobe tumour". Irish Journal of Psychological Medicine. 8 (2): 135–6. doi:10.1017/S0790966700015093.
- ↑ Ogren K, Sandlund M (2007). "Lobotomy at a state mental hospital in Sweden. A survey of patients operated on during the period 1947-1958". Nordic Journal of Psychiatry. 61 (5): 355–62. doi:10.1080/08039480701643498. PMID 17990197.
- ↑ (Burgess, 2003, p. 309).
- ↑ (Burgess, 2003, p. 310).
- ↑ (Stuss, 1999, p. 348; cf. Burgess & Simons, 2005).
- ↑ (cf. Burgess & Simons, 2005).
- ↑ Semendeferi K, Lu A, Schenker N, Damasio H (March 2002). "Humans and great apes share a large frontal cortex". Nature Neuroscience. 5 (3): 272–6. doi:10.1038/nn814. PMID 11850633.
External links
| Wikimedia Commons has media related to Frontal lobe. |