Femoroacetabular impingement
Femoroacetabular Impingement (FAI), or hip impingement syndrome, may affect the hip joint in young and middle-aged adults[1] and occurs when the ball shaped femoral head rubs abnormally[2] or does not permit a normal range of motion in the acetabular socket.[3] Damage can occur to the articular cartilage, or labral cartilage (soft tissue bumper of the socket), or both. Treatment options range from conservative to arthroscopic to open surgery.
Overview
FAI is regarded as a cause of premature hip osteoarthritis[4][5] and is characterized by abnormal contact between the proximal femur and rim of the acetabulum (hip socket). In most cases, patients present with a deformity in the femoral head, or acetabulum, a poorly positioned femoral-acetabular junction, or any or all of the foregoing. A combination of certain factors may predispose to some form of FAI, predominantly, a marginal developmental hip abnormality together with environmental factors such as activities involving recurrent motion of the legs within a supraphysiologic range.[6]
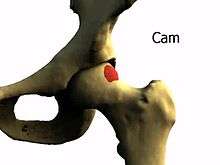
Three types of FAI are recognized. The first involves an excess of bone along the upper surface of the femoral head, known as a Cam deformity. (abbreviation for camshaft which the shape of the femoral head and neck resembles). The second is due to an excess of growth of the upper lip of the acetabular cup and is known as a 'Pincer' deformity. Colloquially, these are referred to as 'Cam' and 'Pincer'. The third is a combination of the two. Studies have suggested that 'Cam' deformities are more common in the male, while 'Pincer' deformities are more common in females. However, the most common situation, approximately 70%, is a combination of both.[7] A complicating issue is that some of the radiographic findings of FAI have also been described in asymptomatic subjects.[8] Consequently, the true frequency of femoroacetabular impingement is currently under debate, but the ultimate result is increased friction between the acetabular cup and femoral head which may result in pain and loss or reduction of hip function.
Diagnosis
FAI-related pain is often felt in the groin, but may also be experienced in the lower back or around the hip.[4] The diagnosis, often with a co-existing labral tear,[9] typically involves physical examination in which the range of motion of the hip is tested. Limited flexibility leads to further examination with x-ray, providing a two-dimensional view of the hip joints. Additional specialized views, such as the Dunn view, may make x-ray more sensitive.[10] Subsequent imaging techniques such as CT or MRI may follow producing a three-dimensional reconstruction of the joint to evaluate the hip cartilage, demonstrate signs of osteoarthritis, or measure hip socket angles (e.g. the alpha-angle as described by Nötzli[11] in 2-D and by Siebenrock in 3-D[12]). It is also possible to perform dynamic simulation of hip motion with CT or MRI [13][14] assisting to establish whether, where, and to what extent, impingement is occurring.
Treatment
The treatment of FAI varies. Conservative treatment includes reducing levels of physical activity, anti-inflammatory medication and physiotherapy. Physical Therapy [physiotherapy] may optimize alignment and mobility of the joint, thereby decreasing excessive forces on irritable or weakened tissues. It may also identify specific movement patterns that may be causing injury.
Due to the frequency of diagnosis in adolescents and young adults, various surgical techniques have been developed with the goal of preserving the hip joint. Surgery may be arthroscopic or open,[4] peri-acetabular or rotational osteotomies being two common open surgical techniques employed when an abnormal angle between femur and acetabulum has been demonstrated. These primarily aim to alter the angle of the hip socket in such a way that contact between the acetabulum and femoral head are greatly reduced, allowing a greater range of movement. Femoral sculpting may be performed simultaneously, if required for a better overall shape of the hip joint. It is unclear whether or not these interventions effectively delay or prevent the onset of arthritis. Well designed, long term studies evaluating the efficacy of these treatments have not been done.[15]
A 2011 study analyzing current surgical methods for management of symptomatic femoral acetabular impingement (FAI), suggested that arthroscopic method had surgical outcomes equal to or better than other methods with a lower rate of major complications when performed by experienced surgeons.[16]
Trivia
Notable persons who suffered hip impingements:
- Charlie Morton, American baseball pitcher[17]
- Devin Mesoraco, Cincinnati Reds catcher[18]
References
- ↑ Dooley PJ (January 2008). "Femoroacetabular impingement syndrome: Nonarthritic hip pain in young adults". Can Fam Physician. 54 (1): 42–7. PMC 2293316
 . PMID 18208954.
. PMID 18208954. - ↑ "Femoroacetabular Impingement (FAI)". Hipfai.com. Retrieved March 18, 2013.
- ↑ https://web.archive.org/web/20100614001312/http://healthcare.utah.edu/orthopaedics/patients/education/femoral.html. Archived from the original on June 14, 2010. Retrieved September 12, 2010. Missing or empty
|title=(help) - 1 2 3 Chakraverty, J.K.; Snelling, N.J. (2012). "Anterior hip pain – Have you considered femoroacetabular impingement?". International Journal of Osteopathic Medicine. 15: 22. doi:10.1016/j.ijosm.2011.09.003.
- ↑ Lung R, O'Brien J, Grebenyuk J, et al. (May 2012). "The prevalence of radiographic femoroacetabular impingement in younger individuals undergoing total hip replacement for osteoarthritis". Clin Rheumatol. 31 (8): 1239–42. doi:10.1007/s10067-012-1981-9.
- ↑ Leunig M, Beaulé PE, Ganz R (March 2009). "The concept of femoroacetabular impingement: current status and future perspectives". Clin. Orthop. Relat. Res. 467 (3): 616–22. doi:10.1007/s11999-008-0646-0. PMC 2635437. PMID 19082681.
- ↑ Beck M, Kalhor M, Leunig M, Ganz R (Jul 2005). "Hip morphology influences the pattern of damage to the acetabular cartilage: femoroacetabular impingement as a cause of early osteoarthritis of the hip". J Bone Joint Surg Br. 87 (7): 1012–8. doi:10.1302/0301-620X.87B7.15203. PMID 15972923.
- ↑ Chakraverty JK, Sullivan C, Gan C, Narayanaswamy S, Kamath S (Feb 2013). "Cam and pincer femoroacetabular impingement: CT findings of features resembling femoroacetabular impingement in a young population without symptoms". Am J Roentgenol. 200 (2): 389–95. doi:10.2214/AJR.12.8546. PMID 23345362.
- ↑ Bedi, A., Chen, N., Robertson, W., & Kelly, B. T. (2008). The management of labral tears and femoroacetabular impingement of the hip in the young, active patient. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 24(10), 1135-1145.
- ↑ Clohisy JC, Carlisle JC, Beaulé PE, Kim YJ, Trousdale RT, Sierra RJ, Leunig M, Schoenecker PL, Millis MB (2008). "Approach to the Plain Radiographic Evaluation of the Young Adult Hip". J Bone Joint Surg Am. 90 Suppl 4: 47–66. doi:10.2106/JBJS.H.00756. PMC 2682767. PMID 18984718.
- ↑ Nötzli HP, Wyss TF, Stoecklin CH, Schmid MR, Treiber K, Hodler J (May 2002). "The contour of the femoral head-neck junction as a predictor for the risk of anterior impingement". J Bone Joint Surg Br. 84 (4): 556–60. doi:10.1302/0301-620X.84B4.12014. PMID 12043778.
- ↑ Siebenrock KA, Ferner F, Noble PC, Santore RF, Werlen S, Mamisch TC (November 2011). "The cam-type deformity of the proximal femur arises in childhood in response to vigorous sporting activity". Clin. Orthop. Relat. Res. 469 (11): 3229–40. doi:10.1007/s11999-011-1945-4. PMC 3183218. PMID 21761254.
- ↑ Tannast M, Kubiak-Langer M, Langlotz F, Puls M, Murphy SB, Siebenrock KA (January 2007). "Noninvasive three-dimensional assessment of femoroacetabular impingement". J. Orthop. Res. 25 (1): 122–31. doi:10.1002/jor.20309. PMID 17054112.
- ↑ http://www.clinicalgraphics.com Dynamic motion simulation for hip impingement.
- ↑ Wall PD, Brown JS, Costa M, Buchbinder R, Griffin DR (2014). "Surgery for Femoroacetbaular Impingement: Cochrane Review". Cochrane Database of Systematic Reviews. 9: CD010796. doi:10.1002/14651858.CD010796.pub2.
- ↑ Matsuda DK, et al. (February 2011). "Comparative Systematic Review of the Open Dislocation, Mini-Open, and Arthroscopic Surgeries for Femoroacetabular Impingement". The Journal of Arthroscopic and Related Surgery. 27 (2): 252–269. doi:10.1016/j.arthro.2010.09.011.
- ↑ http://triblive.com/sports/pirates/7548649-74/morton-mound-surgery#axzz3OQsUcAbN
- ↑ http://mlb.mlb.com/news/article.jsp?ymd=20150505&content_id=122530266&vkey=news_cin&c_id=cin
Further reading
- Lewis CL, Sahrmann SA (January 2006). "Acetabular labral tears". Phys Ther. 86 (1): 110–21. PMID 16386066.
External links
- Femoroacetabular Impingement (FAI) on OrthoInfo
- Hip Impingement Awareness website written by ex FAI patient, Louisa Weeks Browning
- Hip Preservation Awareness, information and support for hip impingement, hip dysplasia, and related issues in young adults (12-adult)
- IMPAKT-HiP (Investigations of Mobility, Physical Activity, and Knowledge in Hip Pain) Study by the Arthritis Research Centre of Canada