Pure tone audiometry
| Pure tone audiometry | |
|---|---|
| Diagnostics | |
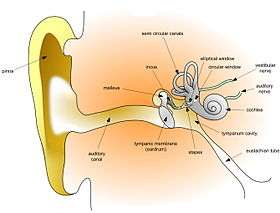 Diagram of the human ear | |
| ICD-9-CM | 95.41 |
| MeSH | D001301 |
Pure tone audiometry (PTA) is the key hearing test used to identify hearing threshold levels of an individual, enabling determination of the degree, type and configuration of a hearing loss.[1] Thus, providing the basis for diagnosis and management. PTA is a subjective, behavioural measurement of hearing threshold, as it relies on patient response to pure tone stimuli. Therefore, PTA is used on adults and children old enough to cooperate with the test procedure. As with most clinical tests, calibration of the test environment, the equipment and the stimuli to ISO standards is needed before testing proceeds. PTA only measures audibility thresholds, rather than other aspects of hearing such as sound localization and speech recognition. However, there are benefits of using PTA over other forms of hearing test, such as click auditory brainstem response (ABR). PTA provides ear specific thresholds, and uses frequency specific pure tones to give place specific responses, so that the configuration of a hearing loss can be identified. As PTA uses both air and bone conduction audiometry, the type of loss can also be identified via the air-bone gap. Although PTA has many clinical benefits, it is not perfect at identifying all losses, such as ‘dead regions’ of the cochlea and neuropathies such as auditory processing disorder (APD).[2][3] This raises the question of whether or not audiograms accurately predict someone’s perceived degree of disability.
PTA procedural standards
There are both international and British standards regarding the PTA test protocol. The British Society of Audiology (BSA) is responsible for publishing the recommended procedure for PTA, as well as many other audiological procedures. The British recommended procedure is based on international standards. Although there are some differences, the BSA-recommended procedures are in accordance with BS EN ISO 8253-1, which is the international standard for PTA established by the International Organization for Standardization. The BSA-recommended procedures provide a "best practice" test protocol for professionals to follow, increasing validity and allowing standardisation of results across Britain. The British Society of Audiology. Recommended Procedure: Pure Tone air and bone conduction threshold audiometry with and without masking and determination of uncomfortable loudness levels.[4]
Variations
There are cases where conventional PTA is not an appropriate or effective method of threshold testing. Procedural changes to the conventional test method may be necessary with populations who are unable to cooperate with the test in order to obtain hearing thresholds. Sound field audiometry may be more suitable when patients are unable to wear earphones, as the stimuli are usually presented by loudspeaker. A disadvantage of this method is that although thresholds can be obtained, results are not ear specific. In addition, response to pure tone stimuli may be limited, because in a sound field pure tones create standing waves, which alter sound intensity within the sound field. Therefore, it may be necessary to use other stimuli, such as warble tones in sound field testing.[5] There are variations of conventional audiometry testing that are designed specifically for young children and infants, such as behavioral observation audiometry, visual reinforcement audiometry and play audiometry.[6][7]
Conventional audiometry tests frequencies between 250 hertz (Hz) and 8 kHz, whereas high frequency audiometry tests in the region of 8 kHz-16 kHz. Some environmental factors, such as ototoxic medication and noise exposure, appear to be more detrimental to high frequency sensitivity than to that of mid or low frequencies. Therefore, high frequency audiometry is an effective method of monitoring losses that are suspected to have been caused by these factors. It is also effective in detecting the auditory sensitivity changes that occur with aging.[8]
Cross hearing and interaural attenuation


When sound is applied to one ear the contralateral cochlea can also be stimulated to varying degrees, via vibrations through the bone of the skull. When the stimuli presented to the test ear stimulates the cochlea of the non-test ear, this is known as cross hearing. Whenever it is suspected that cross hearing has occurred it is best to use masking. This is done by temporarily elevating the threshold of the non-test ear, by presenting a masking noise at a predetermined level. This prevents the non-test ear from detecting the test signal presented to the test ear. The threshold of the test ear is measured at the same time as presenting the masking noise to the non-test ear. Thus, thresholds obtained when masking has been applied, provide an accurate representation of the true hearing threshold level of the test ear.[9]
A reduction or loss of energy occurs with cross hearing, which is referred to as interaural attenuation (IA) or transcranial transmission loss.[9] IA varies with transducer type. It varies from 40 dB to 80 dB with supra-aural headphones. However, with insert earphones it is in the region of 55 dB. The use of insert earphones reduces the need for masking, due to the greater IA which occurs when they are used (See Figure 1).[10]
Air conduction results in isolation, give little information regarding the type of hearing loss. When the thresholds obtained via air conduction are examined alongside those achieved with bone conduction, the configuration of the hearing loss can be determined. However, with bone conduction (performed by placing a vibrator on the mastoid bone behind the ear), both cochleas are stimulated. IA for bone conduction ranges from 0-20 dB (See Figure 2). Therefore, conventional audiometry is ear specific, with regards to both air and bone conduction audiometry, when masking is applied.
PTA thresholds and hearing disability
PTA is described as the gold standard for assessment of a hearing loss.[11] But, how accurate is PTA at classifying the hearing loss of an individual, in terms of hearing impairment and hearing disability? Hearing impairment is defined by the World Health Organisation (WHO) as a hearing loss with thresholds higher than 25db in one or both ears. The degree of hearing loss is classified as mild, moderate, severe or profound.[12] The results of PTA are a good indicator of hearing impairment.
Hearing disability is defined by the WHO as a reduction in ability to hear sounds in quiet and background noise (compared to people with normal hearing), which is caused by a hearing impairment.[13] Several studies have investigated whether self-reported hearing problems (via questionnaires and interviews) were associated with the results from PTA. The findings of these studies indicate that in general, the results of PTA correspond to self-reported hearing problems (i.e. hearing disability). However, for some individuals this is not the case. Therefore, the results of PTA cannot be used to ascertain an individual's hearing disability.[14][15]
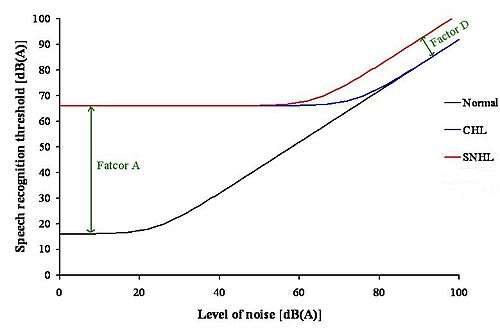
Hearing impairment (based on the audiogram) and auditory handicap (based on speech discrimination in noise) data was reviewed by Reinier Plomp . This led to the formulation of equations, which described the consequences of a hearing loss on speech intelligibility. The results of this review indicated that there were two factors of a hearing loss, which were involved in the effect on speech intelligibility. These factors were named Factor A and Factor D. Factor A affected speech intelligibility by attenuating the speech, whereas Factor D affected speech intelligibility by distorting the speech.[16]
Speech recognition threshold (SRT) is defined as the sound pressure level at which 50% of the speech is identified correctly. For a person with a conductive hearing loss (CHL) in quiet, the SRT needs to be higher than for a person with normal hearing. The increase in SRT depends on the degree of hearing loss only, so Factor A reflects the audiogram of that person. In noise, the person with a CHL has the same problem as the person with normal hearing (See Figure 10).[16]
For a person with a Sensorineural hearing loss (SNHL) in quiet, the SRT also needs to be higher than for a person with normal hearing. This is because the only factor that is important in quiet for a CHL and a SNHL is the audibility of the sound, which corresponds to Factor A. In noise, the person with a SNHL requires a better signal-to-noise ratio to achieve the same performance level, as the person with normal hearing and the person with a CHL. This shows that in noise, Factor A is not enough to explain the problems of a person with a SNHL. Therefore, there is another problem present, which is Factor D. At present, it is not known what causes Factor D. Thus, in noise the audiogram is irrelevant. It is the type of hearing loss that is important in this situation.[16]
These findings have important implications for the design of hearing aids. As hearing aids at present can compensate for Factor A, but this is not the case for Factor D. This could be why hearing aids are not satisfactory for a lot of people.[16]
Audiograms and hearing loss
The shape of the audiogram resulting from PTA audiometry gives an indication of the type of hearing loss as well as possible causes. Conductive hearing loss due to disorders of the middle ear shows as a flat increase in thresholds cross the frequency range. Sensorineural hearing loss will have a contoured shape depending on the cause. Presbycusis or age-related hearing loss for example is characterized by a high frequency roll-off (increase in thresholds). Noise-induced hearing loss has a characteristic notch at 4000hz. Other coutours may indicate other causes for the hearing loss.
See also
- Hearing range
- Auditory masking
- Auditory filters
- Absolute threshold of hearing
- Equal-loudness contours
References
- ↑ Audiology Pure-Tone Testing at eMedicine
- ↑ Moore, BC (April 2004). "Dead regions in the cochlea: conceptual foundations, diagnosis, and clinical applications.". Ear and hearing. 25 (2): 98–116. doi:10.1177/108471380100500102. PMID 15064655.
- ↑ Moore BCJ. Dead Regions in the Cochlea: Diagnosis, Perceptual Consequences, and Implications for the Fitting of hearing aids. Trends Amplif. 2001;5:1-34.
- ↑ The British Society of Audiology. September 2011 amended 2015. http://www.thebsa.org.uk/wp-content/uploads/2011/04/Pure-Tone-Audiometry-1.pdf [Accessed 13/11/2016]
- ↑ http://www.emedicine.com/ent/topic311.htm [Accessed on 27/02/07]
- ↑ http://michiganotoplasty.com/understanding-deafness-pta-testing/ [Accessed on 07/18/15].
- ↑ "Hearing Testing and Screening in Young Children". patient.info. Retrieved 16 November 2014.
- ↑ Monteiro de Castro Silva, I; Feitosa, MA (2005). "High-frequency audiometry in young and older adults when conventional audiometry is normal.". Brazilian journal of otorhinolaryngology. 72 (5): 665–72. doi:10.1590/S0034-72992006000500014. PMID 17221060.
- 1 2 Katz J. Clinical Handbook of Audiology. 5th ed. Philadelphia: Lippincott Williams & Wilkins; 2002.
- ↑ Bagatto, M; Moodie, S; Scollie, S; Seewald, R; Moodie, S; Pumford, J; Liu, KP (2005). "Clinical protocols for hearing instrument fitting in the Desired Sensation Level method.". Trends in amplification. 9 (4): 199–226. doi:10.1177/108471380500900404. PMID 16424946.
- ↑ Sindhusake D, Mitchell P, Smith W, Golding M, Newall P, Hartley D, et al. Validation of self-reported hearing loss. The Blue Mountains Hearing Study. Int. J. Epidemiol. 2001;30:1371-78.
- ↑ "Deafness and hearing loss Fact sheet N°300". WHO (World Health Organization). Retrieved 16 November 2014.
- ↑ "Sound Advice". Sound Advice Safety and Health Ltd. Retrieved 10 May 2016.
- ↑ Hietamen A, Era P, Henrichsen J, Rosenhall U, Sorri M, Heikkinen E. Hearing among 75-year old people in three Nordic localities: A comparative study. Int. J. Audiol. 2004;44:500-08.
- ↑ Uchida Y, Nakashima T, Ando F, Niino N, Shimokata H. Prevalence of Self-perceived Auditory Problems and their Relation to Audiometric Thresholds in a Middle-aged to Elderly Population. Acta. Otolaryngol. 2003;123:618-26.
- 1 2 3 4 Plomp, R (February 1978). "Auditory handicap of hearing impairment and the limited benefit of hearing aids.". The Journal of the Acoustical Society of America. 63 (2): 533–49. doi:10.1121/1.381753. PMID 670550.
External links
- EMedicine.com.
- GPNotebook.co.uk.
- Springerlink.com.
- Audition Cochlea Promenade oreille ear organ Corti C.R.I.C Montpellier. This website provides excellent diagrams and animated pictures that aid understanding of the topics covered. There are a wide range of topics covered including sound, cochlea, Organ of Corti, hair cell pathology and audiometry.
- Audiology Resources. This site provides useful resources for people interested in audiology.
- This site provides excellent information regarding the Audiometric Testing procedure