Keratocystic odontogenic tumour
| Keratocystic odontogenic tumour | |
|---|---|
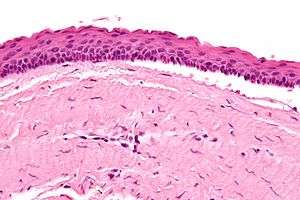 | |
| Micrograph of a keratocystic odontogenic tumour. H&E stain. | |
| Classification and external resources | |
| ICD-10 | D16.4 (Maxilla); D16.5 (mandible) |
| ICD-9-CM | 213.0-213.1 |
A keratocystic odontogenic tumour (also keratocystic odontogenic tumor, KCOT)[1] is a rare and benign but locally aggressive developmental cystic neoplasm. It most often affects the posterior mandible.
It used to be called odontogenic keratocyst (OKC).[1][2]
Diagnosis

The definitive diagnosis is by histologic analysis, i.e. excision and examination under the microscope.
Under the microscope, KCOTs vaguely resemble keratinized squamous epithelium;[3] however, they lack rete ridges and often have an artifactual separation from their basement membrane.
Etiology
KCOTs are thought to arise from the dental lamina and are associated with impacted teeth. Multiple odontogenic keratocysts are a feature of nevoid basal cell carcinoma syndrome. Odotogenic Keratocysts are derived from the remnants of the Dental Lamina.
Genetics
Sporadic (non-syndromic) and syndromic KCOTs are associated with mutations in the gene PTCH, which is part of the Hedgehog signaling pathway.[1][4]
Symptoms
Swelling is the most common presenting complaint; however, KCOTs may be asymptomatic and found incidentally on dental X-rays.[5]
Differential diagnosis
Radiologically
- Odontogenic Myxoma
- Ameloblastoma
- Central Giant Cell Granuloma
Histologically
- Orthokeratocyst
Malignant transformation
Malignant transformation to squamous cell carcinoma may occur, but is unusual.[6]
Treatment

As the condition is quite rare, opinions among experts about how to treat KCOTs differ.
Treatment options:[1]
- Wide (local) surgical excision.
- Marsupialization - the surgical opening of the (KCOT) cavity and a creation of a marsupial-like pouch, so that the cavity is in contact with the outside for an extended period, e.g. three months.
- Curettage (simple excision & scrape-out of cavity).
- Peripheral ostectomy after curettage and/or enucleation.
- Simple excision.
- Carnoy's solution - usually used in conjunction with excision.
- Enucleation and cryotherapy [7]
Additional images
 Intermed. mag.
Intermed. mag. High mag.
High mag. Intermed. mag.
Intermed. mag.
References
- 1 2 3 4 Madras J, Lapointe H (March 2008). "Keratocystic odontogenic tumour: reclassification of the odontogenic keratocyst from cyst to tumour". J Can Dent Assoc. 74 (2): 165–165h. PMID 18353202.
- ↑ Mateus GC, Lanza GH, de Moura PH, Marigo Hde A, Horta MC (November 2008). "Cell proliferation and apoptosis in keratocystic odontogenic tumors" (PDF). Med Oral Patol Oral Cir Bucal. 13 (11): E697–702. PMID 18978709.
- ↑ Thompson LDR. Head and neck pathology - (Foundations in diagnostic pathology). Goldblum JR, Ed.. Churchill Livingstone. 2006. ISBN 0-443-06960-3.
- ↑ PATCHED, DROSOPHILA, HOMOLOG OF, 1; PTCH1. OMIM. URL: http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=601309. Accessed on: December 25, 2008.
- ↑ Habibi A, Saghravanian N, Habibi M, Mellati E, Habibi M (September 2007). "Keratocystic odontogenic tumor: a 10-year retrospective study of 83 cases in an Iranian population". J Oral Sci. 49 (3): 229–35. doi:10.2334/josnusd.49.229. PMID 17928730.
- ↑ Piloni MJ, Keszler A, Itoiz ME (2005). "Agnor as a marker of malignant transformation in odontogenic keratocysts". Acta Odontol Latinoam. 18 (1): 37–42. PMID 16302459.
- ↑ Schmidt BL, Pogrel MA (2001). "The use of enucleation and liquid nitrogen cryotherapy in the management of odontogenic keratocysts.". J Oral Maxillofac Surg. 59: 720–727. doi:10.1053/joms.2001.24278.
Additional reading
- Kahn, Michael A. Basic Oral and Maxillofacial Pathology. Volume 1. 2001.
