Estradiol valerate
 | |
| Clinical data | |
|---|---|
| Pronunciation | ESS-tra-DYE-ole val-er-ate[1] |
| Trade names | Altadiol, Deladiol, Delestrogen, Estraval, Lastrogen, Progynon Depot, Progynova, Valergen, others |
| Routes of administration | Oral, intramuscular injection[2] |
| ATC code | G03CA03 (WHO) |
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Bioavailability |
Oral: 3–5%[3][4] Intramuscular: 100%[3] |
| Metabolism | Cleavage via esterases in the liver, blood, and tissues[3][5] |
| Metabolites | Estradiol, valeric acid,[3][5] and metabolites of estradiol |
| Biological half-life |
Oral: 12–20 hours (as E2)[3][6] Intramuscular: 4–5 days[3] |
| Duration of action | Intramuscular (5 mg): 7–8 days[7] |
| Excretion | Urine (80%)[3] |
| Identifiers | |
| |
| CAS Number | 979-32-8 |
| PubChem (CID) | 13791 |
| ChemSpider | 13194 |
| UNII | OKG364O896 |
| KEGG | D01413 |
| ChEBI | CHEBI:31561 |
| ChEMBL | CHEMBL1511 |
| Chemical and physical data | |
| Formula | C23H32O3 |
| Molar mass | 356.498 g/mol |
| 3D model (Jmol) | Interactive image |
| |
| |
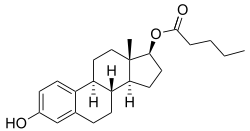
Estradiol valerate (EV, E2V) (INN, USAN, JAN) (brand name Progynova, Progynon Depot, Delestrogen, many others), or oestradiol valerate (BAN), is a synthetic, steroidal estrogen and an estrogen ester – specifically, the 17β-valerate ester of estradiol – which is marketed in the United States, Canada, Europe, and throughout much of the rest of the world.[8][9] It acts as a prodrug of estradiol, and hence, is considered to be a natural, bioidentical form of estrogen.[5] Along with estradiol cypionate, estradiol valerate is one of the most widely used esters of estradiol.[10]
Medical uses
The medical uses of estradiol valerate are the same as those of estradiol and other estrogens. Examples of indications for the drug include hormone replacement therapy and hormonal contraception. In regards to the latter, estradiol valerate is available in combination with a progestogen as an combined estradiol-containing oral contraceptive (with dienogest)[11] and as a combined injectable contraceptive (with hydroxyprogesterone caproate or norethisterone enanthate).[12][13][14]
Side effects
The side effects of estradiol valerate are the same as those of estradiol. Examples of such side effects include breast tenderness and enlargement, nausea, bloating, edema, headache, and melasma.[15]
Pharmacology
The affinity of estradiol valerate for the estrogen receptor is approximately 50 times lower than that of estradiol.[3] In addition, estradiol valerate is rapidly cleaved into estradiol and is unable to reach target tissues in any concentration of significance, if at all.[3] As such, estradiol valerate is essentially inactive in terms of estrogenic effect itself, acting solely as a prodrug to estradiol.[3]
Pharmacokinetics
Upon ingestion, regardless of the route of administration, estradiol valerate behaves as a prodrug via cleavage by esterases into estradiol and the natural fatty acid valeric acid.[3][4][16] This cleavage occurs not only in the liver, but also in the blood and in tissues, and the hydrolysis of estradiol valerate into estradiol and valeric acid is complete regardless of whether the drug is administered orally or parenterally.[3] High levels of circulating estradiol are found after an intravenous injection of estradiol valerate, and this indicates very rapid cleavage of the drug upon entering circulation.[3] In contrast to estradiol, which can distribute into and exert its effects in target tissues, valeric acid is quickly metabolized via beta oxidation (see also fatty acid metabolism).[3]
Oral administration
The esterification of the C17β position of estradiol as in estradiol valerate prevents the metabolism of estradiol valerate by 17β-hydroxysteroid dehydrogenase (17β-HSD).[4] As approximately 80% of estradiol is metabolized into estrone (and estrone sulfate) by 17β-HSD during first-pass metabolism, this improves the metabolic stability and hence bioavailability of estradiol valerate.[5] However, estradiol valerate is hydrolyzed into estradiol and valeric acid in the intestines, and hence, is still subject to extensive (albeit comparatively reduced) first-pass metabolism.[4] As such, the oral bioavailability of estradiol valerate is only around 3 to 5%, and is comparable to that of micronized estradiol (which has similarly improved bioavailability relative to (non-micronized) oral estradiol).[3][4] Due to its nature as a rapidly converted prodrug of estradiol, the pharmacokinetics of estradiol valerate are similar to those of micronized estradiol.[3][4] Moreover, the pharmacodynamics and potency (after differences in molecular weight are taken into account) of oral estradiol valerate are considered to be equivalent to those of micronized estradiol.[3] This is also notably true for effects on hepatic protein synthesis (e.g., of SHBG), again after differences in molecular weight between the two drugs are considered.[3]
A dosage of 1 mg/day oral estradiol valerate has been found to produce approximate circulating concentrations of 50 pg/mL estradiol and 160 pg/mL estrone, while a dosage of 2 mg/day results in circulating levels of 60 pg/mL estradiol and 300 pg/mL estrone.[17] These concentrations of estradiol and estrone are comparable to those observed with 1 and 2 mg/day oral micronized estradiol.[17]
Intramuscular administration
| Estrogen | Peak levels | Time to peak | Duration |
|---|---|---|---|
| Estradiol cypionate | E2: 338 pg/mL E1: 145 pg/mL | E2: 3.9 days E1: 5.1 days | 11 days |
| Estradiol valerate | E2: 667 pg/mL E1: 324 pg/mL | E2: 2.2 days E1: 2.7 days | 7–8 days |
| Estradiol benzoate | E2: 940 pg/mL E1: 343 pg/mL | E2: 1.8 days E1: 2.4 days | 4–5 days |
In contrast to oral administration, the bioavailability of estradiol valerate has been found to be complete (i.e., 100%) via intramuscular injection.[3][4] Due to the far greater bioavailability of intramuscular estradiol valerate relative to oral, the former is substantially stronger (in terms of potency) than the latter.[3] As an example, a single 4 mg intramuscular injection is said to be approximately equivalent to 2 mg/day of the drug administered orally over the course of 3 weeks.[3] Estradiol valerate, when given intramuscularly in oil, has a relatively long duration due to the formation of an intramuscular depot from which the drug is slowly released and absorbed.[3][18] Upon intramuscular injection of estradiol valerate in an oil solution, the solvent (i.e., oil) is absorbed, and a primary microcrystalline depot is formed within the muscle at the site of injection.[4] In addition, a secondary depot may also be formed in adipose tissue.[4] The slow release of estradiol valerate is caused by the increased lipophilicity of the drug, which in turn is due to its long fatty acid valeric acid ester moiety.[3] The terminal half-life of intramuscularly administered estradiol valerate in oil is reported to be 4 to 5 days.[3]
A single intramuscular injection of 4 mg estradiol valerate has been found to result in maximal circulating levels of estradiol of about 390 pg/mL within 3 days of administration, with levels declining to 100 pg/mL (baseline, in the study) by 12–13 days.[19] Another study found that a single intramuscular injection of 5 mg estradiol valerate resulted in peak circulating levels of 667 pg/mL estradiol and 324 pg/mL estrone within approximately 2 and 3 days, respectively (see right/above table).[7] The duration of estradiol valerate at this dose and in this study was considered to be 7 to 8 days.[7] Other studies have found that larger doses of intramuscular estradiol valerate exceeding 20 mg have a duration of more than 15 days.[7] A third study, in contrast to the preceding study, found that a single 10 mg intramuscular injection of estradiol valerate resulted in maximal estradiol levels of 506–544 pg/mL and maximal estrone levels of 205–219 pg/mL in postmenopausal women.[20]
A study of high-dose combined intramuscular administration of 40 mg estradiol valerate and 250 mg hydroxyprogesterone caproate per week for six months (described as a "pseudopregnancy" regimen) in hypogonadal women found that circulating levels of estradiol increased from 27.8–34.8 pg/mL to 3028–3226 pg/mL after three months and to 2491–2552 pg/mL after six months of treatment.[21]
Chemistry
Estradiol valerate is an estrane (C18) steroid and the C17β valerate (or pentanoate) fatty acid ester of estradiol. It is also known as estra-1,3,5(10)-triene-3,17β-diol 17β-pentanoate. Other common esters of estradiol in use include estradiol cypionate, estradiol enanthate, and estradiol acetate, the former two of which are C17β esters of estradiol similarly to estradiol valerate and the latter of which is the C3 acetate ester of estradiol.
History
Estradiol valerate was first introduced in 1954 by Squibb as Delestrogen in the United States,[22][23] and along with estradiol benzoate (1936)[24][25] and estradiol cypionate (1952),[26] has since become one of the most widely used esters of estradiol.[10]
Society and culture
Availability
Oral estradiol valerate is used primarily in Europe, under the brand name Progynova.[27] Although previously available in the United States,[9] estradiol valerate is no longer available in this country in an oral formulation (except in combination with dienogest as a combined oral contraceptive under the brand name Natazia).[28] Intramuscular estradiol valerate is available under the brand name Delestrogen in the U.S.[28] and Canada and under the brand name Progynon Depot in Europe and elsewhere in the world.[9] In the U.S., it is available in formulations of 10 mg/mL, 20 mg/mL, and 40 mg/mL in oil (as Delestrogen, as well as generics).[28] The only other injectable formulations of estrogen available in the U.S. are estradiol cypionate (5 mg/mL in oil) and conjugated estrogens (Premarin) (25 mg/vial in solution).[28]
References
- ↑ https://www.drugs.com/cons/estradiol-and-dienogest.html
- ↑ Christoph Zink (1 January 1988). Dictionary of Obstetrics and Gynecology. Walter de Gruyter. p. 86. ISBN 978-3-11-085727-6. Retrieved 20 May 2012.
- 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 Düsterberg B, Nishino Y (December 1982). "Pharmacokinetic and pharmacological features of oestradiol valerate". Maturitas. 4 (4): 315–24. doi:10.1016/0378-5122(82)90064-0. PMID 7169965.
- 1 2 3 4 5 6 7 8 9 Kuhl H (2005). "Pharmacology of estrogens and progestogens: influence of different routes of administration". Climacteric. 8 Suppl 1: 3–63. doi:10.1080/13697130500148875. PMID 16112947.
- 1 2 3 4 Kuhnz, W.; Blode, H.; Zimmermann, H. (1993). "Pharmacokinetics of Exogenous Natural and Synthetic Estrogens and Antiestrogens". 135 / 2: 261–322. doi:10.1007/978-3-642-60107-1_15. ISSN 0171-2004.
- ↑ Stanczyk, Frank Z.; Archer, David F.; Bhavnani, Bhagu R. (2013). "Ethinyl estradiol and 17β-estradiol in combined oral contraceptives: pharmacokinetics, pharmacodynamics and risk assessment". Contraception. 87 (6): 706–727. doi:10.1016/j.contraception.2012.12.011. ISSN 0010-7824.
- 1 2 3 4 5 Oriowo MA, Landgren BM, Stenström B, Diczfalusy E (April 1980). "A comparison of the pharmacokinetic properties of three estradiol esters". Contraception. 21 (4): 415–24. doi:10.1016/s0010-7824(80)80018-7. PMID 7389356.
- ↑ A. D. Roberts (1991). Dictionary of Steroids: Chemical Data, Structures, and Bibliographies. CRC Press. p. 415. ISBN 978-0-412-27060-4. Retrieved 20 May 2012.
- 1 2 3 Index Nominum 2000: International Drug Directory. Taylor & Francis US. 2000. p. 405. ISBN 978-3-88763-075-1. Retrieved 20 May 2012.
- 1 2 Samuel S. C. Yen (1991). Reproductive endocrinology: physiology, pathophysiology, and clinical management. Saunders. ISBN 978-0-7216-3206-3. Retrieved 20 May 2012.
- ↑ Guida M, Bifulco G, Di Spiezio Sardo A, Scala M, Fernandez LM, Nappi C (2010). "Review of the safety, efficacy and patient acceptability of the combined dienogest/estradiol valerate contraceptive pill". International Journal of Women's Health. 2: 279–90. doi:10.2147/IJWH.S6954. PMC 2990895
 . PMID 21151673.
. PMID 21151673. - ↑ Newton JR, D'arcangues C, Hall PE (1994). "A review of "once-a-month" combined injectable contraceptives". J Obstet Gynaecol (Lahore). 4 Suppl 1: S1–34. doi:10.3109/01443619409027641. PMID 12290848.
- ↑ http://www.wjpps.com/download/article/1412071798.pdf
- ↑ Rowlands, S (2009). "New technologies in contraception". BJOG: An International Journal of Obstetrics & Gynaecology. 116 (2): 230–239. doi:10.1111/j.1471-0528.2008.01985.x. ISSN 1470-0328.
- ↑ Amit K. Ghosh (23 September 2010). Mayo Clinic Internal Medicine Board Review. OUP USA. pp. 222–. ISBN 978-0-19-975569-1.
- ↑ "Progynova 1mg (SPC) | Drugs.com". Retrieved 2012-09-06.
- 1 2 O'Connell MB (1995). "Pharmacokinetic and pharmacologic variation between different estrogen products". J Clin Pharmacol. 35 (9 Suppl): 18S–24S. PMID 8530713.
- ↑ Sriram. Medicinal Chemistry. Pearson Education India. p. 427. ISBN 978-81-317-0031-0. Retrieved 20 May 2012.
- ↑ M. Notelovitz; P.A. van Keep (6 December 2012). The Climacteric in Perspective: Proceedings of the Fourth International Congress on the Menopause, held at Lake Buena Vista, Florida, October 28–November 2, 1984. Springer Science & Business Media. pp. 399–. ISBN 978-94-009-4145-8.
- ↑ Schug BS, Donath F, Blume HH (2012). "Bioavailability and pharmacodynamics of two 10-mg estradiol valerate depot formulations following IM single dose administration in healthy postmenopausal volunteers". Int J Clin Pharmacol Ther. 50 (2): 100–17. PMID 22257576.
- ↑ Ulrich U, Pfeifer T, Lauritzen C (1994). "Rapid increase in lumbar spine bone density in osteopenic women by high-dose intramuscular estrogen-progestogen injections. A preliminary report". Horm. Metab. Res. 26 (9): 428–31. doi:10.1055/s-2007-1001723. PMID 7835827.
- ↑ William Andrew Publishing (22 October 2013). Pharmaceutical Manufacturing Encyclopedia, 3rd Edition. Elsevier. pp. 1477–. ISBN 978-0-8155-1856-3.
- ↑ Larry L. Duetsch (1969). Research and development, market power, and patent policy in ethical drugs. University of Wisconsin--Madison. p. 95.
- ↑ Enrique Raviña; Hugo Kubinyi (16 May 2011). The Evolution of Drug Discovery: From Traditional Medicines to Modern Drugs. John Wiley & Sons. p. 175. ISBN 978-3-527-32669-3. Retrieved 20 May 2012.
- ↑ Folley SJ (December 1936). "The effect of oestrogenic hormones on lactation and on the phosphatase of the blood and milk of the lactating cow" (PDF). The Biochemical Journal. 30 (12): 2262–72. PMC 1263335. PMID 16746289.
- ↑ Marshall Sittig (1 January 1988). Pharmaceutical Manufacturing Encyclopedia. William Andrew. pp. 575–576. ISBN 978-0-8155-1144-1. Retrieved 20 May 2012.
- ↑ Joseph S. Sanfilippo (January 1998). Primary Care in Obstetrics and Gynecology: A Handbook for Clinicians. Springer Science & Business Media. pp. 227–. ISBN 978-0-387-94739-6.
- 1 2 3 4 "Drugs@FDA: FDA Approved Drug Products". United States Food and Drug Administration. Retrieved 12 October 2016.